Keywords:
Education and training, Education, Conventional radiography, Musculoskeletal bone, Bones
Authors:
A. L. Proenca, A. P. Caetano, L. Bogalho; Lisbon/PT
DOI:
10.1594/essr2017/P-0209
Imaging findings OR Procedure Details
There are multiple lines and angles described in hip radiographic evaluation which provide diagnostic clues for several disorders (congenital,
acquired or degenerative).
|
Lines and Angles for Radiographic Evaluation of Hip Joint
|
|
1.
Acetabular index
|
|
2.
Alpha angle
|
|
3.
Center-edge angle of Wiberg
|
|
4.
Femoral neck angle (CCD angle)
|
|
5.
Hip joint space
|
|
6.
Ilioischial line (Köhler line)
|
|
7.
Iliopectineal line
|
|
8.
Shenton´s line
|
|
9.
Skinner’s (femoral angle) line
|
|
10.
Teardrop distance
|
|
11.
Tönnis angle
|
1.
Acetabular index (or Acetabular angle of Sharp)
- Indication: Measures acetabular inclination or opening and evaluates acetabular depth in potential developmental dysplasia of the hip.
- Projection: Anteroposterior pelvic view.
- Measurement: Angle formed between an horizontal line at the inferior aspect of both pelvic teardrops (A) and a line from the inferior margin of the teardrop to the lateral margin of acetabular roof (B).
- Criteria: Angle of intersection should not exceed standards based on age.
In adults,
the normal range is 33-38º.
Angle above 47º suggests acetabular dysplasia and neuromuscular disorders.
Values between 39-46º are indeterminate.
Shallow angle is seen in Down syndrome and achondroplasia.
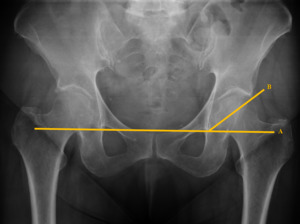
Fig. 15: Acetabular angle
2. Alpha Angle
- Indication: Evaluation of anterior femoral head-neck junction shape in the assessment of femoroacetabular impingement.
- Projection: Cross-table lateral view of the hip.
- Measurement: Angle between a line along the femoral neck axis (A) and a line from the center of the femoral head to the transition of the femoral head into the femoral neck (neck radius exceeds head radius) (B).
- Criteria: Normal angle <55º.
If > 55 degrees then associated with CAM type femoroacetabular impingement.
Nowadays this angle is more used in MRI.

Fig. 16: Alpha angle
3.
Center-edge angle of Wiberg (or Lateral centre-edge (LCE) angle)
- Indication: Assess superolateral coverage provided by acetabular roof.
Evaluation of residual hip dysplasia in children and adults.
- Projection: Anteroposterior pelvic view.
- Measurement: Angle formed between a vertical line through the center of the femoral head (A) and a line from the center of the femoral head,
passing through the most superolateral margin of the acetabulum (B).
- Criteria: Normal angle must be above 25 degrees.
Values of 20-25º are considered borderline.
Elevated angles are associated with protusio acetabuli,
but this is not the most accurate measurement method.
Angle <20º is diagnostic of hip dysplasia.
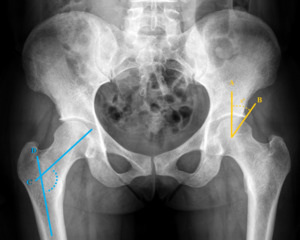
Fig. 17: Center-edge angle of Wiberg (yellow) and Femoral angle (blue)
4.
Femoral neck angle (or Caput-collum-diaphyseal angle (CCD angle))
- Indication: Evaluate hip alignment.
- Projection: Anteroposterior pelvic view.
- Measurement: Angle formed between the lines along the axis of femoral neck (C) and shaft (D)
- Criteria: Normal angle if intersection about 125 degrees.
Coxa vara- angle less than 120 degrees.
Coxa valga - angle more than 130 degrees.
Fig. 17
5.
Hip joint space
- Indication: Evaluation of hip joint space.
- Projection: Anteroposterior pelvic view.
- Measurement: Distance between the cortex of the femoral head and the acetabulum,
superiorly (s),
axially (a) and medially (m).
- Criteria: Distance should not exceed 6 mm superiorly (s),
7 mm axially (a),
or 13 mm medially (m).
Wider distance is associated with hip joint effusion.
The superior joint space is usually reduced by degenerative diseases.
The axial space is commonly narrowed by inflammatory arthritis.
The medial space is affected by both.

Fig. 18: Normal hip joint spaces: s –superior, a – axial, m - medial

Fig. 19: Patient with ostheoarthritis showing reduced hip spaces, more pronounced in the superior and medial joint space.
6.
Ilioischial line (or Köhler’s line)
- Indication: Evaluation of posterior column of the pelvis.
- Projection: Anteroposterior pelvic view.
- Measurement: Line along the outer border of the obturator foramen to the medial border of the iliac wing.
It should pass through the acetabular teardrop.
- Criteria: Medial acetabular wall should not extend medially to this line.
Coxa profunda - medial acetabular wall extended medial to the ilioischial line.
Protusio acetabuli – acetabulum and femoral head projected medial to ilioischial line.
Protusio acetabuli can be primary or secondary to rheumatoid or degenerative arthritis,
Paget’s disease,
osteogenesis imperfecta,
and idiopathic or other bone-softening disorders.
If line is disrupted,
consider posterior column fracture of the acetabulum.

Fig. 20: Ilioischial line (yellow) and iliopectineal line (green)
7.
Iliopectineal line
- Indication: Evaluation of anterior column.
- Projection: Anteroposterior pelvic view.
- Measurement: A linear bony ridge extending from the medial border of the iliac wing,
along the superior border of the superior pubic ramus,
ending at the pubic symphysis,
defining the anterior column of the pelvis.
- Criteria: Smooth and continuous line.
If disrupted,
consider anterior column fracture of the acetabulum.
Thickening of this line is associated with Paget disease,
familial idiopathic hyperphosphatasia,
metabolic or neoplasic conditions.
Fig. 20
8.
Shenton’s hip line
- Indication: Evaluation of femoral neck integrity and alignment.
- Projection: Anteroposterior pelvic view.
- Measurement: Line along the inferior border of the superior pubic ramus and inferomedial border of the femural neck.
- Criteria: Smooth and continuous line.
Disruption of this line is associated with hip dislocation,
femoral neck fracture,
and slipped capital femoral epiphysis.
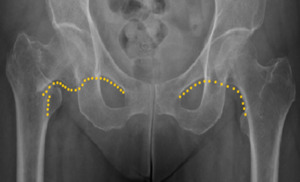
Fig. 22: Left – Intact Shenton´s line.
Right - Disruption of Shenton´s line in a transtrochanteric fracture.
9. Skinner’s line
- Indication: Assessment of relationship of the fovea capitis to the trochanteric line.
- Projection: Anteroposterior pelvic view.
- Measurement: Line along the longitudinal femoral shaft axis (A).
Perpendicular line tangential to the tip of the greater trochanter (B).
- Criteria: The perpendicular line should pass through or below the fovea capitis.
Hip joint abnormality if line is found above the fovea capitis; suspect fracture or bone-softening conditions causing coxa vara.

Fig. 23: Skinner´s line
10. Teardrop distance
- Indication: Useful to evaluate for hip joint effusion or for hip dysplasia.
- Projection: Anteroposterior pelvic view.
- Measurement: Distance between medial aspect of the femoral head and the lateral edge of the pelvic teardrop.
- Criteria: Distance should not exceed 11mm.
Contralateral side should not differ more than 2mm.
Waldenström’s sign - discrepancy between and right and left teardrop distance is >2mm.
Wider distance is a non-specific sign of hip joint effusion.
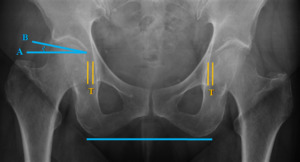
Fig. 24: Symmetrical Teardrop distance (yellow). Tönnis angle (blue)
11.
Tönnis angle (or Index of the Weightbearing Zone or Horizontal toit externe (HTE) angle)
- Indication: Measures inclination of weight bearing zone (acetabular roof),
giving an indirect measure of femoral incongruence.
- Projection: Anteroposterior pelvic view.
- Measurement: Angle formed between a horizontal running through the most inferior point of the sclerotic acetabular sourcil (A) and a line extending from the medial to lateral edges of the sourcil (B).
- Criteria Normal: 0-10º.
Measurement greater than 10° is a radiographic sign of hip dysplasia.
Acetabuli with increased Tönnis angles are subject to structural instability,
whereas those with decreased Tönnis angles are at risk for Pincer type femoroacetabular impingement.
Fig. 24
Salvar
Salvar



 and Femoral angle (blue)")


 and iliopectineal line (green)")



. Tönnis angle (blue)")